
Bridging the Gap: Lessons from a Safety-Critical Elements Audit
In the world of process safety, Safety Critical Elements (SCE) are the invisible sentinels standing between normal operations and catastrophe. These are the pieces of equipment, systems, or software whose failure could contribute to a major accident or whose purpose is to prevent or limit its consequences. Identifying and managing these elements throughout their entire lifecycle is one of the most significant challenges industrial organizations face today.
RskLess recently completed a comprehensive gap analysis of a facility’s Critical Control Management (CCM) program. While the facility had made measurable progress, our audit revealed the common "Reactive" state that many organizations find themselves in. By examining the process, our findings, and the resulting recommendations, we can gain insight into how to move from a reactive culture to one of operational excellence.
The Gravity of SCE Failure: A Historical Context
Before diving into the audit details, it is essential to recognize why this work is so serious. History is a stern teacher, and major incidents are almost always preceded by the failure of Safety Critical Elements.
Take, for instance, the 2005 BP Texas City refinery explosion. This disaster, which resulted in 15 deaths and 180 injuries, was a direct consequence of SCE failures. During a unit startup, a raffinate splitter tower was overfilled because level indicators provided false readings, redundant high-level alarms failed to sound, and the blowdown system was an antiquated design that lacked a flare to safely contain and combust flammables.
When SCEs fail during high-risk periods like unit startups which are ten times more likely to result in an incident than normal operations the margin for error vanishes.
The Audit Process: A Deep Dive into Process and People
RskLess approaches gap analysis as more than just a documentation review. It is a systematic assessment of the people, processes, and technology required to keep a facility safe.
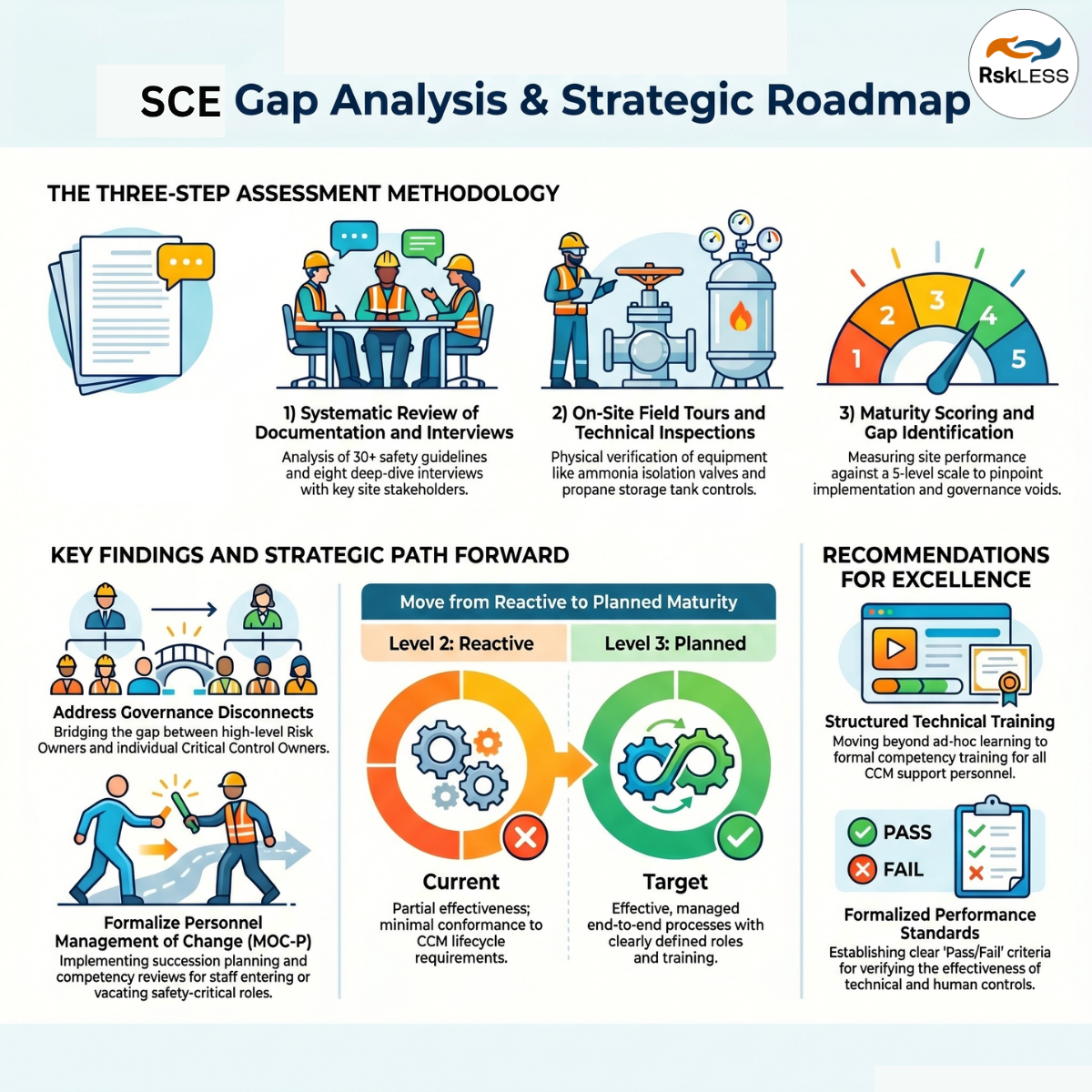
Our recent audit process followed a structured methodology:
Documentation Review: We analyzed over 30 master documents, including Guidelines for SCM Selection, Bowtie reports, Process Hazard Analysis (PHA) data, and maintenance records.
Stakeholder Interviews: We conducted deep-dive interviews with eight key roles, including HSE personnel, engineering planners, shift supervisors, and site leadership.
Field Tour: We facilitated field inspections with operations and maintenance personnel to see how critical controls were managed "at the valve".
Maturity Assessment: We evaluated the facility against a 1-to-5 maturity scale, ranging from Level 1 (Regressive) to Level 5 (Operational Excellence).
This process allowed us to identify not just what was missing, but why certain processes were failing to gain traction in daily operations.
Key Findings: The Challenges of SCE Management
Many organizations struggle with SCEs because management systems often exist in silos. Our audit identified four major areas for improvement:
1. Governance and Responsibility
We found that while a Critical Control Committee existed, it was largely inactive. Furthermore, there was a lack of clarity between "Risk Owners" (typically senior management) and "Critical Control Owners" (those responsible for specific hardware or procedures). Without a well-defined RASCI (Responsible, Accountable, Supporting, Consulted, Informed) chart, accountability for the SCE lifecycle remains fragmented.
2. Identification Disconnects
A common gap is the disconnect between risk assessment data (like PHAs or Bowties) and the field-level Critical Risk Matrix. In our audit, we found that a recent project involving isolation valves on a hazardous system did not result in those valves being identified as critical controls in the site's maintenance software (SAP). If an SCE isn't identified in the system, it doesn't get the specialized maintenance it requires.
3. The "Intuition" Trap in Maintenance
In many reactive organizations, the repair prioritization of equipment is based on informal intuition rather than clear criticality thresholds. If a device isn't flagged as "Safety Critical" in the maintenance system, its failure might be treated as routine, leading to dangerous delays in restoring a primary layer of protection.
4. The Human Factor: Management of Change (MOC)
While technical MOC is often strong, Management of Change for Personnel (MOC-P) is frequently overlooked. We found no formal process to ensure that when a Critical Control Owner vacates their position, their knowledge and accountability are effectively transferred to a successor.
Recommendations: The Path to Excellence
While the findings were serious, the path forward is optimistic. Moving from Level 2 (Reactive) to Level 3 (Planned) is achievable through a focused end-to-end process.
Our key recommendations included:
Formalize the Committee: Reactivate the Critical Control Committee with integrated representation from management, Process Safety (PSM), and maintenance to ensure major accident hazards are jointly managed.
Integrate PHA Data: Ensure a standardized methodology for using PHA and LOPA data to automatically identify and flag SCEs in maintenance systems.
Establish Performance Standards: Define clear "pass/fail" criteria for SCE effectiveness so that owners can move away from intuition-based decisions toward data-driven assurance.
Targeted Training: Move away from ad-hoc, "learn-on-the-fly" training. Critical Control Owners and executors need structured, technical training on the significance of the systems they manage.
Conclusion: Safer Than Yesterday
Managing Safety Critical Elements is a daunting task, but it is the cornerstone of preventing catastrophic loss. By acknowledging these real challenges from governance gaps to human factor complexities, organizations can begin the hard work of systematic improvement.
At RskLess, our goal is to help you bridge these gaps, ensuring that your layers of protection are not just checkboxes on a form, but robust, verified, and safer than yesterday.